Image credit: Deemerwha studio | stock.adobe.com
Patient experience data (PED) are no longer a nice to have; it is emerging as a critical component in the development and commercialization of new medicines,1 valued particularly by regulators in defining the efficacy, safety, and value of new medicines.2,3
The cornerstone of PED is understanding the patient’s experiences with disease, treatment, and care, which is best accomplished through qualitative research.4 Many qualitative papers have been published in the past decade to explore patients’ experiences of disease and treatment.5,6 It has become standard practice to present these concepts in a conceptual model.7
In general, these conceptual models show how disease- and treatment-related signs and symptoms impact a patient’s functional status, health perception, quality of life, and outlook. Conceptual models of disease are useful representations of a patient experience of disease and treatment, and are oft used as the basis from which trial endpoints are defined.8
This is both a practical and patient-focused approach to medication development and should be enthusiastically encouraged. However, current models lack a complexity that can lead researchers to ignore other important variables in a clinical trial influencing the patient experience.
Clinical trials are designed to directly measure the effect of a treatment on outcomes. By their design it is assumed that a change in these outcomes is a function of the treatment provisioned. However, there are many other important patient experience variables that may influence outcomes.9
To truly evaluate the impact of treatment on outcomes we need to understand, define, and measure these other variables in clinical trials. Doing so will further help us to translate the findings from clinical trials to a routine clinical (commercial) setting in which the environment is much less controlled. The purpose of the conceptual model of disease is to qualitatively characterize the patient experience, which will serve as the basis for how outcome measurement approach is defined; therefore, it makes sense to expand the conceptual model to include these other patient experience variables that influence outcome measurement.
In this brief paper, we present a three-part framework for a more comprehensive conceptual model of patient experience and propose that qualitative research should seek to explore all aspects of this to provide a more rounded understanding of patient experiences in clinical trials and beyond.
As alluded to above, most conceptual models describe patients’ experiences of disease and treatment, emphasizing and exploring the burden of living with disease, and highlighting the unmet needs conferred by current care from a patient’s perspective.
Such conceptual models are often formulated on a framework offered by Wilson and Cleary10 and expanded by Valderas and Alonso.11 This framework purports that the biologic/physiologic signs and experienced symptoms of a disease and the signs and symptoms associated with treatment can impact directly on daily functioning, which in turn, impacts perceptions of health and health-related quality of life.
Using this framework qualitative PED researchers can seek to understand patients’ experiences, and plot these on a causal pathway from clinical presentations to quality of life.12 Within the framework researchers can also seek to understand the priorities, preferences and needs of patients.13
By identifying the incidence, severity, frequency and bother of signs, symptoms, and functional impacts in a group of patients, researchers can build an understanding of the process by which quality of life is impaired and hypothesize whether and how an improvement in one sign/symptom would confer a benefit to patients’ lives and life quality.14
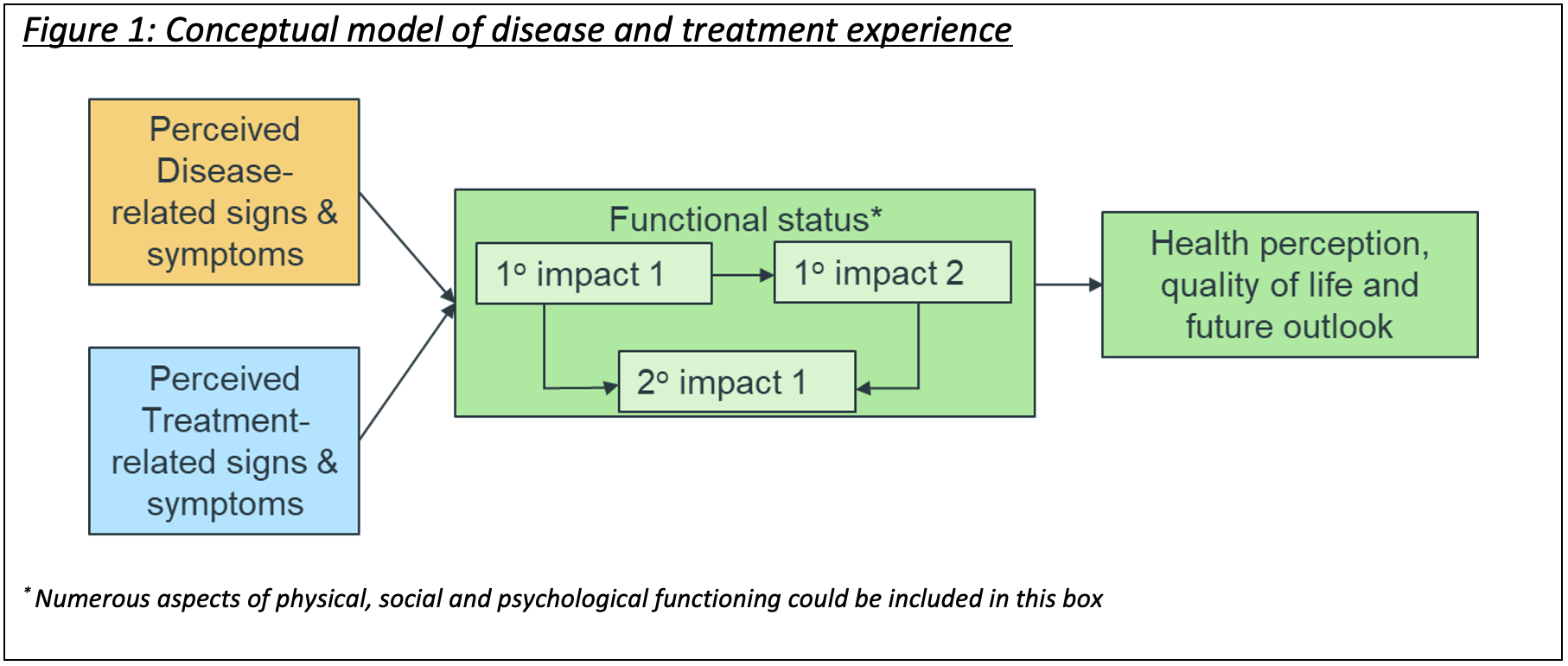
An outline of a typical conceptual model of disease and treatment is shown in Figure 1.
Figure 1: Conceptual model of disease and treatment experience
It has long been known that personal and environmental factors (e.g., demographic characteristics, knowledge, attitudes, beliefs, persona, and social environment) influence patients’ experiences of disease and treatment.15-17 Indeed, Wilson and Cleary included two factors in their model that speak to these at a high level—characteristics of the individual (personal factors) and characteristics of the environment (environmental factors).10
However, these are under-explored in qualitative PED research, and are usually absent from conceptual models of disease and treatment, which are published in the medical and healthcare literature (indeed, they are notably missing from Figure 1, intended to represent the structure of most published conceptual models).
Some researchers have tried to push for the inclusion of these factors into conceptual models18-23 but detailed exploration of these factors in qualitative PED research is rare. This may be because the traditional approaches of obtaining qualitative PED, namely one-on-one interviews and focused groups are ill equipped to capture these factors.
Yet in the era of patient-focused medication development,2,3 and where an emphasis has been placed on diversity, inclusion, and equity in medication development and clinical care,24 these are important to understand as potential moderators and/or mediators of the patient experience with disease and treatment.
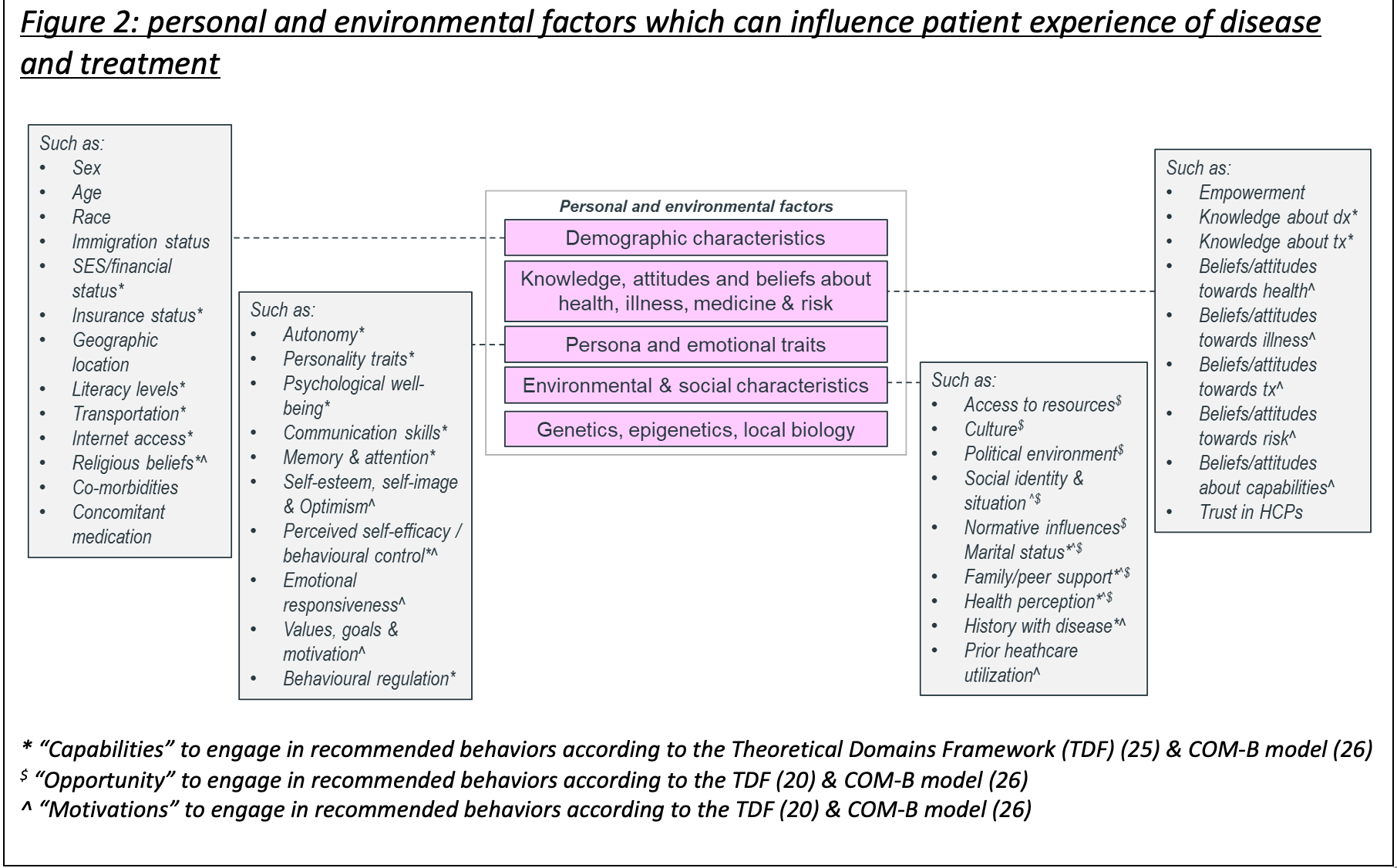
Figure 2 provides some further information about personal and environmental factors, which could be considered in more expansive conceptual models of disease and treatment. Mixed-methods approaches to data generation, including ethnographic methods, anthropological-type observations, and surveys, may be better suited to exploring such factors with patients.
Figure 2: Personal and environmental factors which can influence patient experience of disease and treatment
Experiences with disease and treatment arguably also extend beyond the simple framework put in place by Wilson and Cleary,10 and followed for most conceptual models of disease and treatment (Figure 1). There are other important experiences and interactions that people have within the healthcare system, which will affect their signs, symptoms, functioning, quality of life, and treatment decisions.
These prior experiences may include diagnosis (including prior experience of disease pre-diagnosis, and a patient’s pathway to diagnosis), care encounters, healthcare support (including information from and discussions with their healthcare team and patient communities), and treatment decisions. They may also be receiving their care and treatment within in the context of a clinical trial, which may be a different and more controlled environment from their usual healthcare interactions.
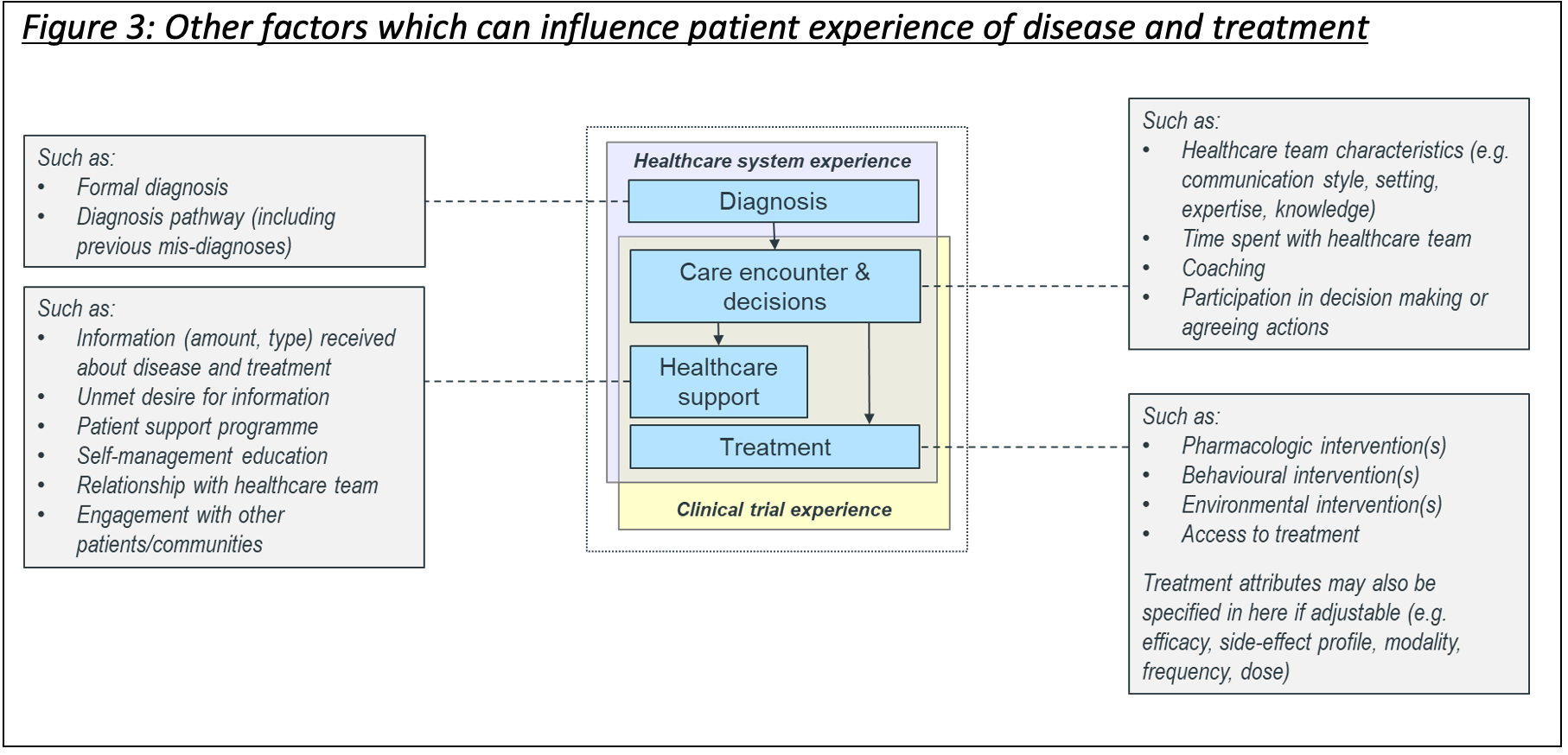
These experiences have been shown to impact the way that people engage with treatment, their self-efficacy in managing their disease in routine clinical care, and clinical effectiveness (Figure 3).27 Care experiences are also important in a clinical trial as their experience with decision-making and their clinical team in that trial will, in turn, impact their experiences of disease and treatment throughout the trial.
Patient perceptions, expectations, motivations, and emotional responses will also invariably impact the way that a patient experiences disease and treatment.28 This is true in clinical care certainly, but could also inform whether someone chooses to participate in a clinical trial, and how well they will engage in/adhere to the protocolized procedures of that trial.29
Again, these are absent in most conceptual models of disease and treatment, despite being prominent in health psychology models for predicting and understanding behavior change and in the medical social science literature, which has shown the interrelations between these factors and patient experience of disease, treatment, and clinical trials.30-33
Personal and environmental factors and prior experiences can collectively be described as enablers and constrainers of positive patient experiences with disease, treatment, and care. It is important to better understand these to both contextualize the patient experiences contained within the conceptual model of disease (Figure 1), and to understand non-medication variables that may determine medication success in a clinical trial.
Figure 3: Other factors which can influence patient experience of disease and treatment
Patient experiences need to be placed into the context of a patient’s own behaviour (present and past), free-will and personal choice.34 However, behavioral decisions made by a patient about the management of their disease is a further element missing in most conceptual models, which emphasize only the signs, symptoms, and impacts on functioning and quality of life associated with disease and treatment (Figure 1).
However, it is important to know how people behave based on how they feel about their treatment and care, how they manage their disease, whether they adhere to recommended treatment, and what other coping mechanisms they use to function and reduce the impact of disease on quality of life. This is especially true in instances of chronic illness or where there are likely other previous treatment experiences35 shaping how they perceive their current disease state and treatment options (Figure 4).
Figure 4: Perceptions and behaviors related to disease management
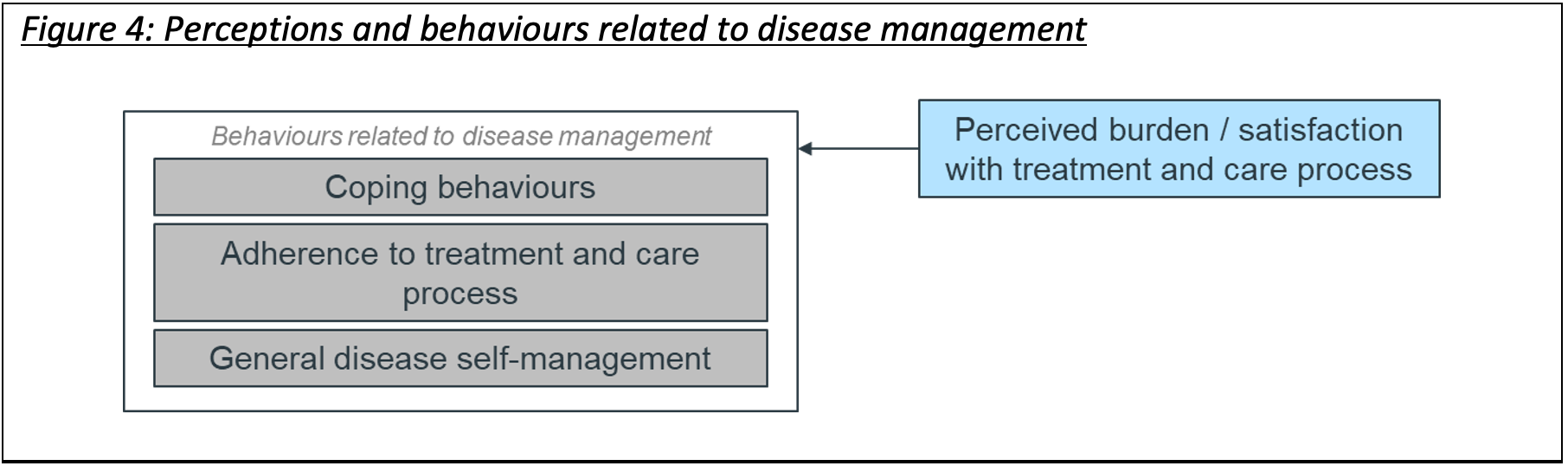
This information can help researchers to understand in more detail some of the challenges people living with disease face, how they manage to cope with it (or not), and the factors that will influence that. This, in turn, can help to predict how people will engage with treatment in trial and routine care contexts.36 For example, patients’ perceived burden/satisfaction with treatment will impact adherence, which alongside other disease-management behaviors (such as lifestyle adaptation for coping, and general disease management) will further impact their perspectives, priorities, needs, and experiences.
As such, exploring patient perceptions of treatment/care and behavioral response are fundamental to comprehensively understanding patient experiences with disease and treatment. It also affords an understanding as to the translational nature of the trial findings to routine care.
A conceptual model of patient experience
Although presented as three separate parts of a framework for a comprehensive conceptual model of patient experiences, there are likely some interdependencies and relationships between them. Combining these three parts into a comprehensive conceptual model of patient experience, therefore, is important, with hypothesized relationships that can be tested through research.
A draft model is shown in Figure 5, adapted from an original publication by Krupnick and Kelly.7 This model can help to inform patient engagement initiatives to increase participation and satisfaction in clinical research,37 can provide the basis for comprehensive qualitative PED research, which seeks to expand understanding of the patient experiences to inform medicines development,38 and can help in defining appropriate clinical care decisions, including the provision of resources for altering contextual factors.34
Figure 5: A draft comprehensive conceptual model of patient experience (adapted from [5])
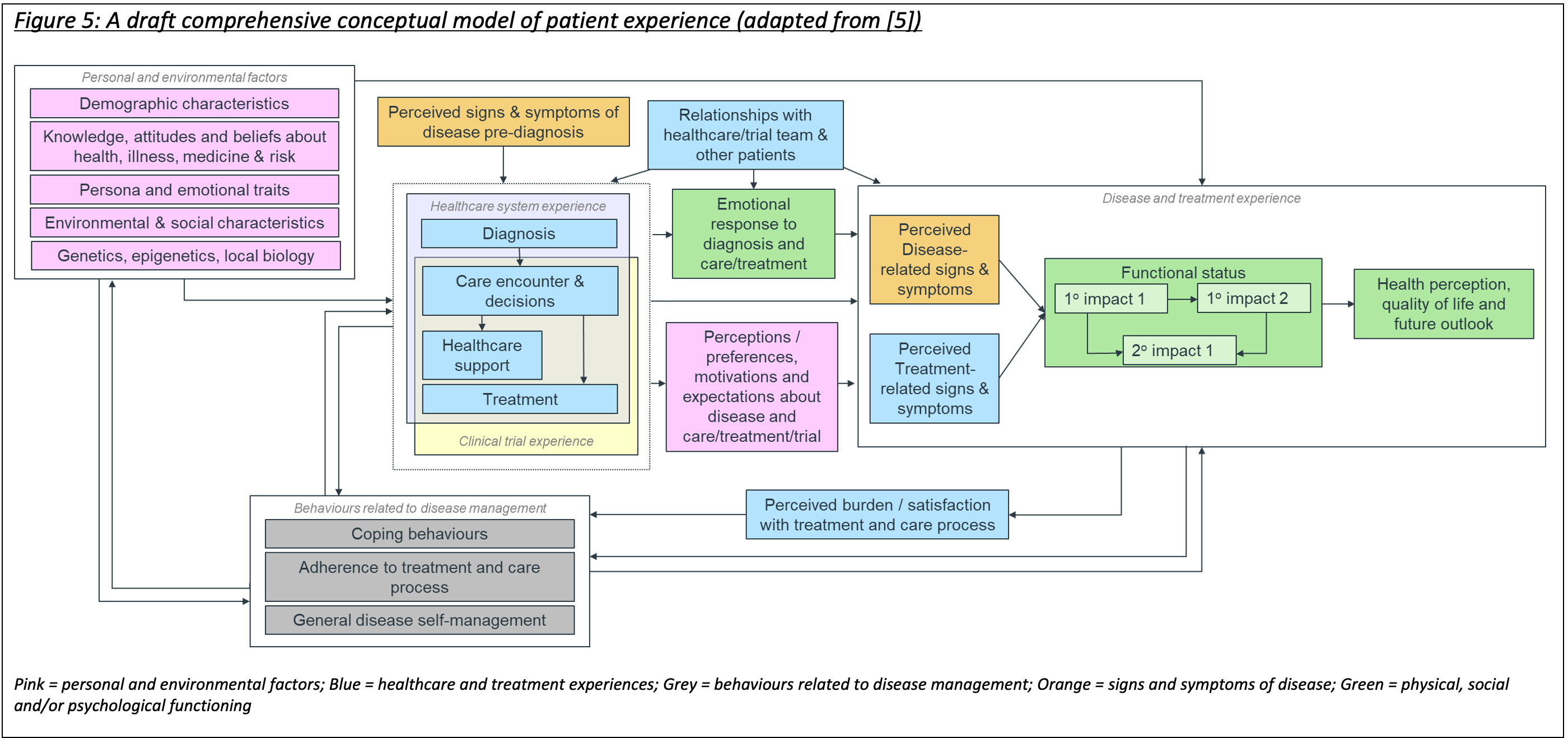
Through this approach, clinical research can better contribute to making more effective treatments available to more people who can benefit from them most.
References
- Reaney M (2023). Patient experience data (PED) in intervention development – what is it, why should you care, and how can this book help? In Reaney M (ed.) Using Patient Experience Data to Evaluate Medical Interventions. Generating, understanding and using patient experience data within and alongside clinical trials.
- U.S. Food and Drug Administration (FDA) Center for Drug Evaluation and Research (CDER). Patient Focused Drug Development. https://www.fda.gov/drugs/development-approval-process-drugs/cder-patient-focused-drug-development (accessed May 2024).
- Patient Focused Medicines Development. https://patientfocusedmedicine.org/(accessed May 2024).
- Oehrlein EM, Burcu M, Schoch S, Gressler LE (2023). Enhancing Patient Centricity of Real-World Data Research: An Exploratory Analysis Using the Patient Experience Mapping Toolbox. Value in Health, 26(1):10-17.
- Renjith V, Yesodharan R, Noronha JA, Ladd E, George A (2021). Qualitative Methods in Health Care Research. International Journal of Preventive Medicine, 12:20.
- Husbands S, Mitchell PM, Coast J (2020). A Systematic Review of the Use and Quality of Qualitative Methods in Concept Elicitation for Measures with Children and Young People. Patient, 13(3):257-288.
- Krupnick R, Kelly K (2023). Understanding patient experiences through qualitative research. In Reaney M (ed.) Using Patient Experience Data to Evaluate Medical Interventions. Generating, understanding and using patient experience data within and alongside clinical trials.
- Patrick DL, Burke LB, Gwaltney CJ, Leidy NK, Martin ML, Molsen E, et al (2011). Content validity—establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO good research practices task force report: part 1—eliciting concepts for a new PRO instrument. Value in Health, 14(8):967–77.
- Reaney M (2014). The importance of understanding the impact of preference in clinical trials of diabetes interventions. Journal of Diabetes, 6(6):496-498.
- Wilson IB, Cleary PD (1995). Linking clinical variables with health-related quality of life. JAMA, 273:59–65.
- Valderas JM, Alonso J (1998).Patient reported outcome measures: a model-based classification system for research and clinical practice. Quality of Life Research, 17:1125-1135.
- Kanters TA, Redekop WK, Rutten-Van Mölken MP, Kruijshaar ME, Güngör D, van der Ploeg AT, et al (2015). A conceptual disease model for adult Pompe disease. Orphanet Journal of Rare Diseases, 15;10:112.
- Aronson KI, Danoff SK, Russell AM, Ryerson CJ, Suzuki A, Wijsenbeek MS, et al (2021). Patient-centered outcomes research in interstitial lung disease: an official American Thoracic Society research statement. American Journal of Respiritary and Critical Care Medicine, 204:e3–e23.
- Guillemin I, Darpelly M, Wong B, Ingelgård A, Griebsch I (2024). Development of a disease conceptual model of patient experience with metastatic colorectal cancer: identification of the most salient symptoms and impacts. Journal of Cancer Survivorship, 18(3):761-771.
- Lock M (1993). Encounters with Aging: Mythologies of Menopause in Japan and North America. Berkeley: University of California Press.
- Adams V (2013). Evidence based global public health. In Biehl J & Petryna A (eds.) When People Come First: Critical Studies in Global Health. Princeton, NJ: Princeton University Press.
- Stronks K, Wieringa NF, Hardon A (2013). Confronting diversity in the production of clinical evidence goes beyond merely including under-represented groups in clinical trials. Trials, 14:177.
- Patrick DL, Chiang YP (2000). Measurement of health outcomes in treatment effectiveness evaluations: conceptual and methodological challenges. Medical Care, 38(9 Suppl):II14-II25.
- Reaney M, Bush EN, Curtis B, Black P, van Brunt K, Gwaltney C (2015). One Programme, Four Stakeholders: An Overview of the Utilisation of Patient-Reported Outcomes in Intervention Development to Meet the Needs of Regulators, Payers, Healthcare Professionals and Patients. Pharmaceutical Medicine, 29:69-78.
- Rodríguez AM, Mayo NE, Gagnon B (2013). Independent contributors to overall quality of life in people with advanced cancer. British Journal of Cancer, 108:1790–1800.
- World Heath Organization (2001). The International Classification of Functioning, Disability and Health (ICF). Available at: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed May 2024).
- Solar O, Irwin A (2010). A conceptual framework for action on the social determinants of health. Social Determinants of Health Discussion Paper 2 (Policy and Practice).Available at: https://www.who.int/publications/i/item/9789241500852(accessed May 2024).
- Kehr J (2016). The Precariousness of Public Health: On Tuberculosis Control in Contemporary France. Medical Anthropology, 35(5):377-89.
- U.S. Food and Drug Administration (FDA). Diversity Plans to Improve Enrollment of Participants from Underrepresented Racial and Ethnic Populations in Clinical Trials Guidance for Industry (draft guidance). https://www.fda.gov/media/157635/download(accessed May 2024).
- Atkins L, Francis L, Islam R, O’Connor D, Patey A, Ivers N, et al (2017).A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implementation Science, 12:77.
- Michie, S., Van Stralen, M. M., & West, R. (2011). The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science, 6:1.
- Doyle C, Lennox L, Bell D (2013). A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open, 3:e001570.
- McCarron TL, Noseworthy T, Moffat K, Wilkinson G, Zelinsky S, White D, et al (2019). Understanding the motivations of patients: A co-designed project to understand the factors behind patient engagement. Health Expectations, 22(4):709-720.
- Bower P, King M, Nazareth I, Lampe F, Sibbald B (2005). Patient preferences in randomised controlled trials: conceptual framework and implications for research. Social Science and Medicine, 61(3):685–695.
- Gilbert H (2013). Re-visioning Local Biologies: HIV-2 and the Pattern of Differential Valuation in Biomedical Research. Medical Anthropology, 32(4):343–358.
- Lock M (2013). The Epigenome and Nature/Nurture Reunification: A Challenge for Anthropology. Medical Anthropology, 32(4):291–308.
- Gibbon S (2017). Entangled local biologies: genetic risk, bodies and inequities in Brazilian cancer genetics. Anthropology & Medicine, 24(2):174-188.
- Armitage CJ, Conner M (2000). Social cognition models and health behaviour: A structured review. Psychology & Health, 15(2):173–189.
- Wade DT, Halligan PW (2004). Do biomedical models of illness make for good healthcare systems? BMJ, 329(7479):1398-1401.
- Büssing A, Ostermann T, Neugebauer EA, Heusser P (2010). Adaptive coping strategies in patients with chronic pain conditions and their interpretation of disease. BMC Public Health, 10:507.
- Cane J, O’Connor D, Michie S (2012).Validation of the theoretical domains framework for use in behaviour change and implementation research. Implementation Science, 7:37.
- Domecq JP, Prutsky G, Elraiyah T, Wang Z, Nabhan M, Shippee N, et al (2014). Patient engagement in research: a systematic review. BMC Health Services Research, 14:89.
- Brady SS, Brubaker L, Fok CS, Gahagan S, Lewis CE, Lewis J, et al (2020). Prevention of Lower Urinary Tract Symptoms (PLUS) Research Consortium. Development of Conceptual Models to Guide Public Health Research, Practice, and Policy: Synthesizing Traditional and Contemporary Paradigms. Health Promotion Practice, 21(4):510-524.
- Geissler PW (2013). Public secrets in public health: Knowing not to know while making scientific knowledge. American Ethnologist, 40(1):13–34